

Quick Summary
- Vaccines train the immune system by preparing it to recognise pathogens before infection occurs. Immune protection depends on complex interactions between innate immunity, adaptive immunity, antibodies, and memory cells.
- New developments such as mRNA vaccines and research on trained immunity are reshaping scientific understanding of how immune memory functions. Vaccination does not always prevent infection, but significantly reduces severe disease, hospitalisation, and mortality.
- The article examines how vaccine responses are measured, why immunity varies between individuals, and what current limitations still shape vaccine research.
This is an autogenerated brief. Please read the entire article.
Few biological encounters have shaped human history more subtly than surviving disease. Long before immunity became measurable in laboratories, societies had already observed its effects in uneven patterns of survival. Thucydides, writing about the plague of Athens, noticed that those who recovered could tend to the sick without falling ill again. Centuries later, Ottoman inoculation practices would travel through diplomatic correspondence into England, while exposure itself increasingly came to be understood not simply as danger, but as a form of biological instruction. Vaccination emerged from this slowly accumulating recognition, that is, the body can be altered by encounter long before it understands what it has encountered.
Vaccination is now routine, part of childhood immunisation schedules, travel requirements, and large-scale public health programmes. The World Health Organization estimates that vaccines prevent between 3.5 and 5 million deaths each year, yet what they actually change in the body remains an area of considerable interest for researchers.
The immune system is often described as the body’s defence mechanism, and notably, as a dynamic system capable of learning from prior exposures. Each encounter with a pathogen leaves behind a trace, allowing the body to respond more effectively the next time. Vaccination builds on this capacity by preparing the immune system in advance, introducing it to selected features of a pathogen without exposing the body to the risks of disease (Pollard & Bijker, 2021).
What is less often examined is how uneven this process can be. The immune system does not operate as a fixed mechanism with predictable outcomes.
It functions as a layered system in which response, memory, and adaptation depend on how multiple processes interact. At a basic level, immunity is organised through two interconnected systems: innate and adaptive immunity. The innate immune system responds first, reacting quickly and recognising general features shared by many pathogens. When a vaccine enters the body, this system detects its components and initiates signalling pathways that recruit other immune cells, and this early phase sets the conditions for what follows. When it is weak, the rest of the immune response is often limited, which means the response does not begin fully formed but is shaped from its earliest stage.
Recognition and the Formation of Response
The adaptive immune system develops more slowly but with greater specificity, identifying particular features of a pathogen and building a targeted response. Dendritic cells play a central role in this process by capturing fragments of the vaccine antigen, processing them, and presenting them to T cells in lymphoid organs. This step allows the immune system to recognise what it has encountered in a form that can be acted upon later, and in research settings the efficiency of this process often determines the strength and durability of the immune response, whether one is working with viral proteins, recombinant constructs, or multiepitope vaccines (Clem, 2011).
Once adaptive immunity is activated, B cells and T cells take on distinct roles. B cells produce antibodies that bind to pathogens and limit their spread, while T cells perform a wider range of functions, with helper T cells (CD4⁺) coordinating immune responses and cytotoxic T cells (CD8⁺) eliminating infected cells. A fraction of both cell types differentiates into memory cells that remain in the body long after the antigen has been cleared. These memory populations are often taken as the basis of long-term protection, sometimes lasting for years or even decades (Pulendran & Ahmed, 2011), and they give the impression of a stable sequence in which exposure leads to recognition, recognition leads to memory, and memory leads to protection. In practice, however, this sequence is less orderly than it appears, since memory is not simply retained but shaped, reinforced, and sometimes limited by the conditions under which it forms.
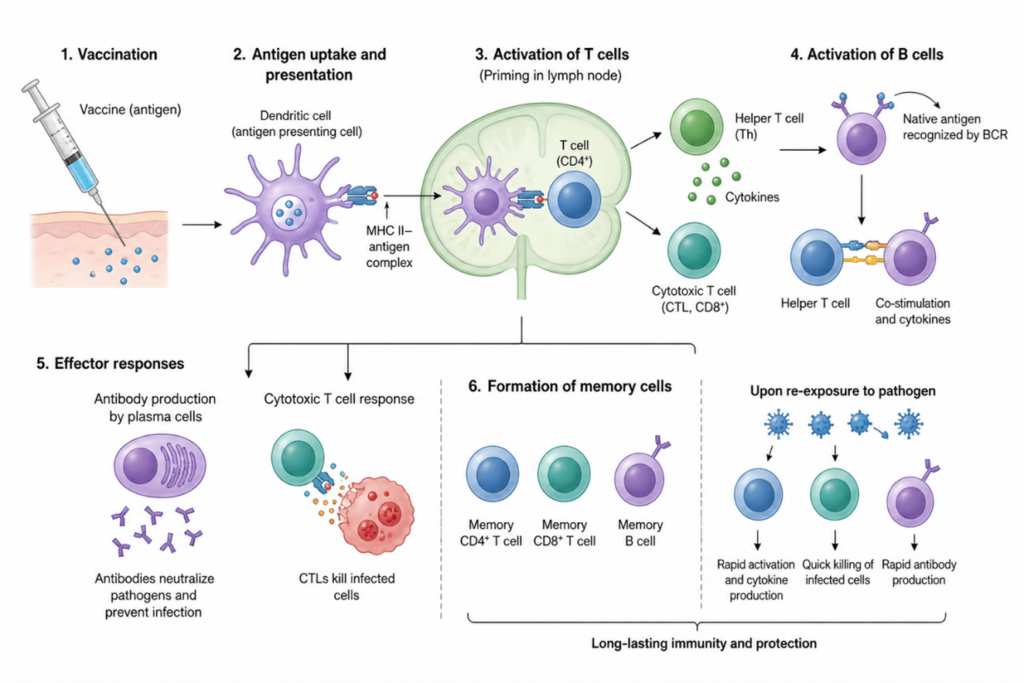
Activation of the immune system following vaccination.
This becomes visible in real-world outcomes. Vaccination does not always prevent infection, but it changes what follows. During the COVID-19 pandemic, for instance, vaccinated populations consistently showed lower rates of severe disease, hospitalisation, and death compared to unvaccinated groups, even when infections continued to occur. What changes is not simply whether the virus enters the body, but how the body handles it.
Designing and Shaping Immune Responses
Vaccines are designed to simulate infection by introducing antigens in a controlled form, allowing the immune system to respond without the risks associated with disease. In applied vaccinology, this makes design central, since selecting antigenic regions that can generate strong neutralising antibody responses while also activating T cell immunity directly affects how well a vaccine performs (Iwasaki & Omer, 2020). This balance is not inherent to the immune system itself but is achieved through careful adjustment of multiple variables, including antigen selection, delivery strategy, and immune signalling, which means that what appears as a biological response is often the result of deliberate design.
Recent developments in vaccine technology have made these adjustments more visible. mRNA vaccines, for example, do not deliver the antigen directly but provide genetic instructions that allow host cells to produce it internally. This changes how the immune system encounters the antigen and often leads to stronger immune activation. From a laboratory perspective, the host effectively becomes the system that produces the antigen, allowing the immune response to develop in a way that more closely resembles natural infection (Pardi et al., 2018), and this shift complicates earlier distinctions between exposure and simulation. The rapid global deployment of mRNA vaccines during COVID-19, with billions of doses administered within a short period, also demonstrated how these laboratory approaches translate into large-scale public health interventions.
Rethinking Memory and Measurement
At the same time, newer research has begun to challenge earlier assumptions about immune memory. Memory was traditionally associated with adaptive immunity, but more recent studies suggest that innate immune cells can also undergo functional changes after exposure to certain vaccines. This process, referred to as trained immunity, allows these cells to respond more efficiently to later challenges, even when those challenges differ from the original pathogen (Montgomery & Larbi, 2025). The immune system appears less divided than previously thought, and the boundaries between immediate response and long-term adaptation become less stable.
These developments raise a broader question about what is actually being retained within the immune system. The success of a vaccine depends not only on generating memory but on the quality and durability of that memory, which includes circulating antibodies, memory B cells, and different subsets of memory T cells. Although antibody levels may decline over time, memory cells can persist and respond rapidly upon re-exposure, which is why vaccinated individuals often experience reduced severity of disease even when infection occurs (Terreri et al., 2022). This also explains why booster doses are sometimes required, not to create immunity from the beginning, but to reinforce and extend existing immune memory.
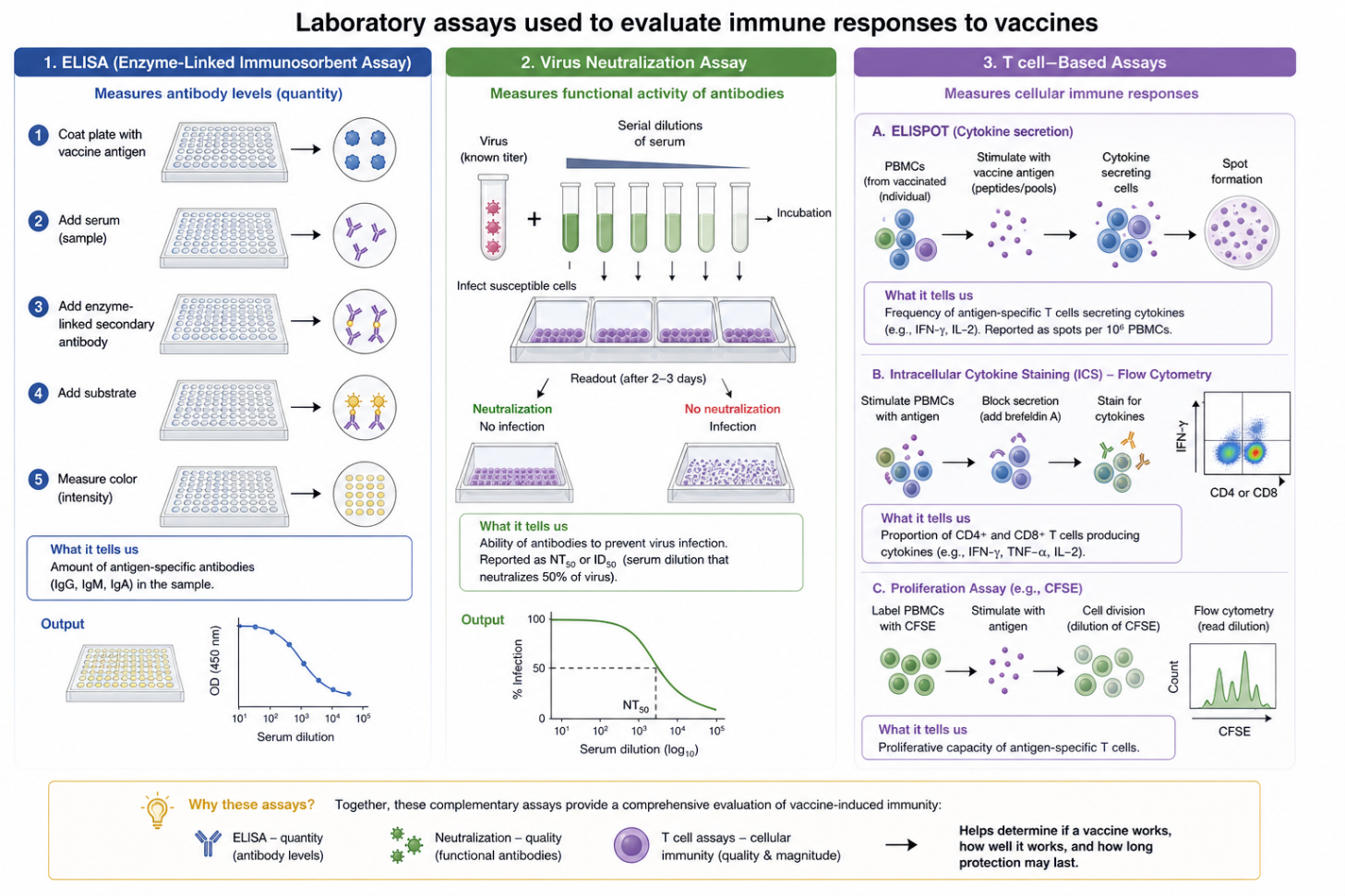
In laboratory settings, these processes are studied by using different techniques. Antibody levels can be measured using ELISA, which quantifies how much antibody is present, while neutralisation assays evaluate the functional capacity of these antibodies to inhibit infection. Cellular responses are studied using T cell-based assays, including ELISpot and intracellular cytokine staining, which measure how immune cells respond to specific antigens. Each method measures a specific component of the immune response, and no single assay fully captures how immunity develops or persists. Therefore, conclusions about immunity depend on how these measurements are interpreted. These assessments are not only academic; they directly inform vaccine approval, updates, and public health recommendations.
Challenges and Future Perspectives
Adjuvants are incorporated into vaccines to enhance immunogenicity, particularly for subunit or peptide-based antigens. They primarily act by activating innate immune pathways, thereby promoting effective antigen presentation and robust adaptive immune responses. The selection of an adjuvant can markedly influence both the magnitude and quality of the immune response, especially in experimental systems (Zhao et al., 2023), underscoring that vaccine-induced immunity is actively modulated rather than inherently uniform.
Despite advances in understanding and technology, limitations remain. Some viruses evolve rapidly, altering their antigenic structure and reducing immune recognition, while others enter through mucosal surfaces where generating strong immunity remains difficult. These challenges continue to shape vaccine development and define the limits of current approaches (Goel et al., 2021).
This is why vaccines for some diseases require frequent updates, while others provide long-term protection with relatively few doses.
The sequence of immune activation following vaccination is often represented schematically, with antigen-presenting cells capturing vaccine antigens, presenting them to T cells, and initiating a cascade that leads to antibody production and cellular responses. A subset of activated cells becomes long-lived memory cells, forming the basis of future immune responses. This sequence is widely accepted, but it represents an idealised model rather than a uniform outcome. Similarly, methods used to evaluate vaccine-induced immunity provide complementary but incomplete information. ELISA quantifies antibody levels, neutralisation assays measure functional antibody activity, and T cell-based assays assess cellular immune responses. Together, these approaches offer a structured assessment of immune function; however, each captures only a specific component. As a result, observations remain partial, and conclusions depend on the interpretation of these combined measurements.
Vaccines prepare the immune system by inducing functional reprogramming rather than simply storing information. Immune responses are dynamic and shaped by prior exposure, host variability, and vaccine design. Consequently, vaccine-induced immunity is not uniform. Vaccination modulates the likelihood, magnitude, and quality of the response, thereby influencing disease severity and protection upon subsequent exposure.

Muttahir Aman
Muttahir Aman is a doctoral researcher in Biotechnology at the University of Kashmir, working in the Vaccine Biotechnology Lab at SKUAST-K. His research focuses on avian virology and vaccinology, particularly the development of cross-protective vaccines against circulating strains, with current work on chimeric vaccine platforms for Infectious Bronchitis Virus. He has trained in molecular and cellular techniques including PCR, qPCR, and flow cytometry, and has contributed to research published in journals such as Archives of Microbiology and Infection. Alongside his academic work, he mentors students and runs a YouTube channel, StudyBits, where he shares biotechnology-related content.

